

Background. The majority of hematopoietic stem cell (HSC) transplants are performed using peripheral blood mobilized with granulocyte-colony stimulating factor (G-CSF) given over 5 days. The goal of a successful transplant is to reliably mobilize optimal numbers of HSCs necessary for rapid and consistent multilineage engraftment. Infusion of mobilized allogeneic grafts results in significant acute and chronic graft-versus-host disease (GvHD) in up to 80% of allogeneic transplant recipients. A reliable and rapid method to mobilize HSC-rich grafts with reduced GvHD potential would be clinically meaningful.
In a Phase 1 study of normal volunteers, MGTA-145 (GroβT), a CXCR2 agonist, when combined with plerixafor, a CXCR4 inhibitor, robustly and rapidly mobilized sufficient HSCs for a safe transplant after only a single day of dosing and apheresis/collection. Here, we phenotypically and functionally profile these mobilized grafts obtained from human volunteers and show that MGTA-145 + plerixafor mobilizes grafts with >10-fold higher engraftment potential (as measured by SCID-repopulating units in NSG mice), a marked reduction in xenogeneic GvHD, and enhanced overall survival compared to G-CSF or plerixafor alone grafts.
Results. In healthy donors, a peak of 40 CD34+ cells/μL were mobilized with MGTA-145 + plerixafor (n=12 donors). 11 of 12 (92%) of these donors mobilized >20 CD34+ cells/μL with single day dosing compared to only 8 of 14 (57%) achieving the same CD34+ cell target treated with plerixafor alone. Eight donors were mobilized with a single dose of MGTA-145 + plerixafor and apheresed on the same day. A median of 4x106 (1.5-7.0x106) CD34+ cells/kg were obtained (n=8 donors) from a median 20 (13-20) L collection. 35.8 (18.5-40.9)% of these cells were CD90+CD45RA-, a CD34+ subset enriched for HSCs, compared to only 6.9 (5.3-9.0)% with G-CSF (p<0.001, n=3 donors). Mechanistically, MGTA-145 bound to CXCR2 on neutrophils and led to a modest and transient increase in plasma concentrations of matrix metalloproteinase 9 (MMP- 9), a downstream target on neutrophils.
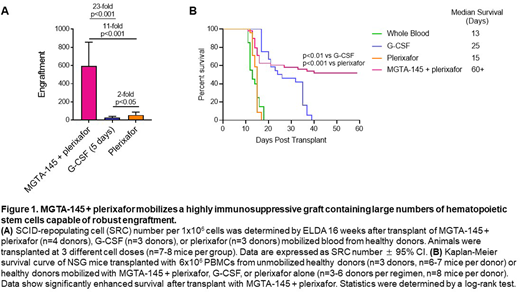
To assess engraftment, we transplanted mobilized peripheral blood cells from healthy donors after a 5-day regimen of G-CSF or a single dose of plerixafor alone or MGTA-145 + plerixafor at limit dilution into sublethally irradiated primary and secondary NSG mouse recipients (n=3 cell doses, n=7-8 mice/group). Multilineage human engraftment was measured by flow cytometry 16 weeks post-transplant and SCID-repopulating cell (SRC) number was calculated (Figure 1A). MGTA-145 + plerixafor mobilized grafts (n=4 donors) led to a 23-fold increase in engraftment compared to G-CSF mobilized grafts (p<0.001, n=3 donors) and 11-fold higher engraftment compared to plerixafor mobilized grafts (p<0.001, n=3 donors).
Immune cell subsets (B, T, and NK cells and cell subsets) mobilized by MGTA-145 + plerixafor were similar to those mobilized by plerixafor alone. While CD3+ T-cell numbers were comparable between MGTA-145 + plerixafor and plerixafor alone, MGTA-145 + plerixafor mobilized 0.2 (0.0-0.6) x108/kg CD8+ T-cells, constituting 1.8 (0.5-4.8)% of the graft, a number and proportion significantly lower than that mobilized by either G-CSF or plerixafor alone.
To determine the effect of the mobilization regimen on xenogeneic GvHD, we developed a xenograft GvHD model in NSG mice where 6x106 PBMCs from various graft sources were infused into sublethally-irradiated animals (n=3-6 donors per graft source). Notably, MGTA-145 + plerixafor mobilized grafts resulted in significantly less GvHD than G-CSF (p<0.01) or plerixafor (p<0.001) grafts (Figure 1B). In vivo cellular subset depletion studies suggested that the GvHD protective effect in MGTA-145 + plerixafor grafts may be in part due to immunosuppressive monocytes which were not present, or present to a lesser degree, in grafts from donors mobilized with G-CSF or plerixafor.
Conclusions. These data demonstrate that MGTA-145 + plerixafor is a rapid, reliable, and G-CSF free method to obtain high numbers of HSCs with durable engraftment potential and a graft with highly immunosuppressive properties. These data suggest that MGTA-145 + plerixafor is an effective single-day mobilization/collection regimen for both autologous and allogeneic stem cell transplantation resulting in enhanced engraftment and reduced GvHD in this xenograft model.
Goncalves:Magenta Therapeutics: Current Employment, Current equity holder in publicly-traded company, Patents & Royalties. Hyzy:Magenta Therapeutics: Current Employment, Current equity holder in publicly-traded company. Hammond:Magenta Therapeutics: Current Employment, Current equity holder in publicly-traded company. Falahee:Magenta Therapeutics: Current Employment, Current equity holder in publicly-traded company. Howell:Magenta Therapeutics: Current Employment, Current equity holder in publicly-traded company. Pinkas:Magenta Therapeutics: Current Employment, Current equity holder in publicly-traded company. Schmelmer:Magenta Therapeutics: Current Employment, Current equity holder in publicly-traded company. Hoggatt:Magenta Therapeutics: Consultancy, Current equity holder in publicly-traded company. Scadden:Magenta Therapeutics: Consultancy, Current equity holder in publicly-traded company, Membership on an entity's Board of Directors or advisory committees. Devine:Magenta Therapeutics: Consultancy. DiPersio:Magenta Therapeutics: Membership on an entity's Board of Directors or advisory committees. Savage:Magenta Therapeutics: Current Employment, Current equity holder in publicly-traded company. Davis:Magenta Therapeutics: Current Employment, Current equity holder in publicly-traded company.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal